Disclaimer: This information is not a substitute for medical care. Always inform your healthcare team of any concerning symptoms you are experiencing, and consult with your provider before starting new treatments, therapies, or health routines.
Why Sexual Pain Happens After Cancer, and What Can Be Done
If you experience discomfort with sexual activity, you’re not alone. Sexual pain happens to be the most commonly reported sexual complaint for women after cancer (Bober & Krapf, 2021). Sometimes referred to as dyspareunia, painful sex can vary from mildly uncomfortable to wildly debilitating. This type of pain can be an acute (early onset) side effect of some cancer treatments, or it can develop as a late-effect. Either way, symptoms can worsen over time if they’re not addressed.
Let’s review some of the common causes for pain with sexual activity after cancer, as well as some strategies available to prevent and manage this problematic survivorship issue. The name of the game should be pleasure, not pain!
Sexual Pain After Cancer Might Be Related To…
Changes in hormone levels.
Estrogen loss is the most likely cause of discomfort with sexual activity after cancer (American Cancer Society, 2021). Premenopausal levels of estrogen contribute to a happy, healthy, vulvovaginal environment by promoting blood flow to the area and keeping the vaginal tissues stretchy and well-lubricated.
Chemotherapy, endocrine therapy (such as tamoxifen, aromatase inhibitors, or ovarian suppression), pelvic radiation, and surgical removal of your ovaries (oophorectomy), can all lead to a sudden drop in estrogen production and cause bothersome menopausal symptoms. Low estrogen levels contribute to vulvovaginal changes such as tissue thinning, loss of elasticity, and dryness, which can lead to irritation and pain with sexual activity.
Changes after pelvic surgery or radiation.
When healing after pelvic surgery or radiation, vaginal tissues can develop fibrosis and scarring. This reduces the stretchy, elastic characteristics that help to make sex comfortable, and can cause the vagina to become shorter and narrower (called vaginal stenosis). Pelvic surgery and radiation can also damage the nerves and blood supply to the reproductive organs and genitals, contributing to vaginal dryness and altered genital sensation.
Graft-Versus-Host Disease (GVHD).
Women who undergo allogeneic hematopoietic stem cell transplants are at risk for developing GVHD, a condition where the transplanted cells attack and damage a person’s organs and tissues. GVHD can affect the tissues of the genitals and reproductive tract. Symptoms may be mild or more severe, and can include vulvovaginal dryness, inflammation, and pain with sexual activity. Over time, vaginal stenosis may develop. Vulvovaginal GVHD requires different types of management than some other causes for sexual pain. Ask your care team if this could be a cause of your symptoms.
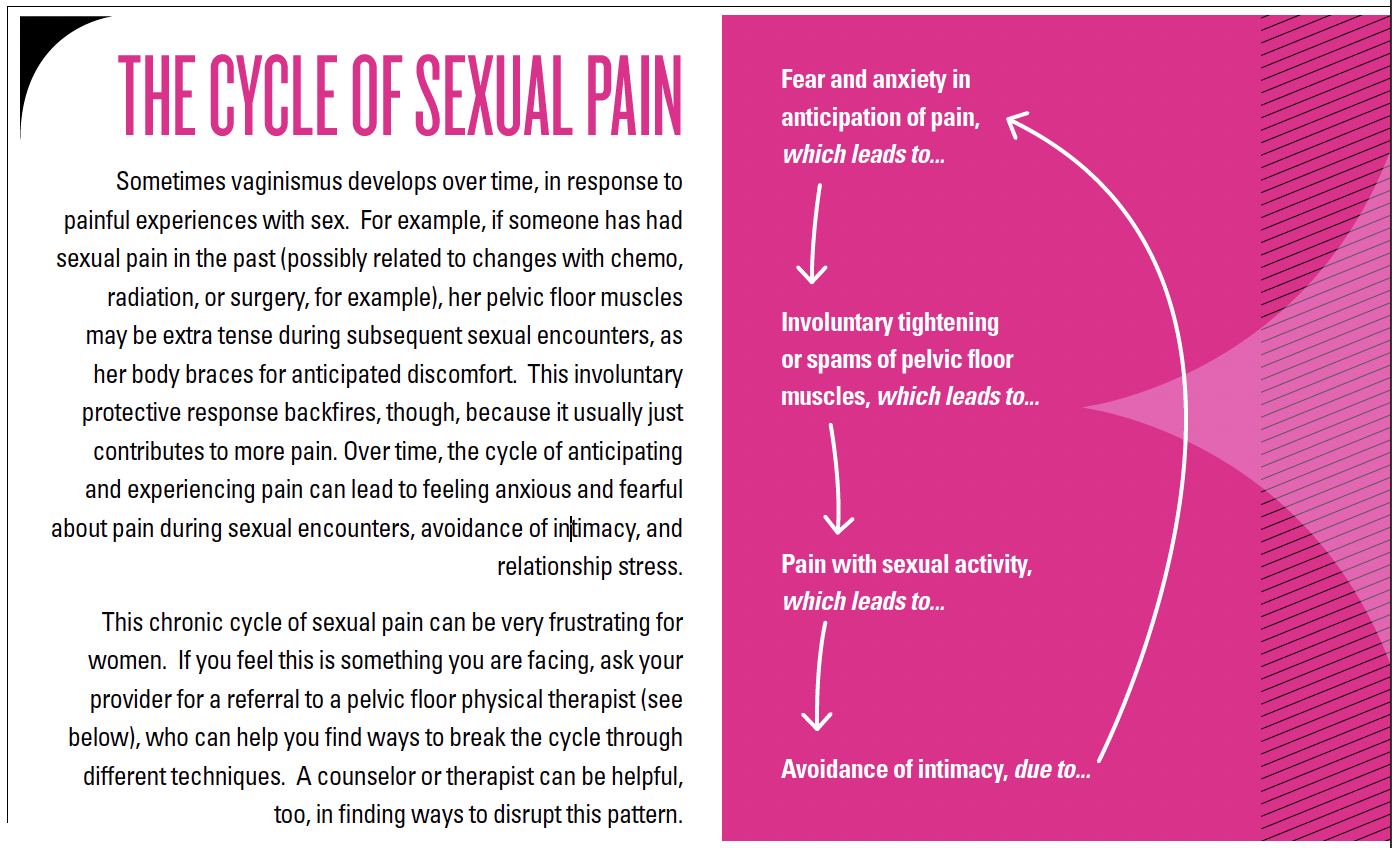
Muscle tension and spasm.
The pelvic floor muscles stretch from our tailbone to our pubic bone, creating a supportive muscular structure for our pelvic organs. This group of muscles also surrounds the vaginal and urethral openings and the anus, playing an important role in control of the bladder and bowel, as well as sexual function. Just like other muscles, pelvic floor muscles can become injured, weakened, chronically tense (hypertonic), or experience spasms. The term vaginismus is sometimes used to describe the involuntary contractions of these muscles that make vaginal penetration during sex difficult, or even impossible. If you’ve ever had a painful cramp in your calf muscle, it’s like that, but in your genitals – ouch!
Strategies for Successfully Overcoming Sexual Pain
Ask your provider for a thorough assessment and physical examination.
Deciphering the reasons for discomfort with sex can be a bit tricky, because there are often multiple factors at play. Plus, different causes of pain require different types of treatment. The expertise of a professional is important for making sure that your symptoms are being managed appropriately.
Once you report your symptoms, your nurse or provider will probably ask for some details. Would you describe the pain as soreness, burning, stabbing, shooting, tingling? Is it generalized or localized? Is it more external (vulvar) or internal (pelvic or vaginal)? When does it start, and how long does it last? What seems to help, and what seems to make it worse?
A physical examination should also be completed, and additional laboratory tests or imaging exams may be ordered based on findings of the assessment and exam. For example, sometimes urinary tract infections (UTIs), sexually transmitted infection (STIs), and yeast infections can contribute to sexual pain. These underlying conditions should either be ruled out or treated.
Simple adjustments to your sexual routine can help.
First, it’s important to communicate with your partner about what you are experiencing and when, as well as what makes your symptoms better or worse. Genital sensation may have changed with cancer treatment, and you and your partner may need to explore how new types of touch make you feel.
Also, always make sure you’re adequately aroused before attempting vaginal intercourse. Your body’s sexual arousal response (the changes that help make penetration comfortable, like increased vaginal lubrication and expansion of the vaginal canal), can take longer after cancer treatments. Slowing down and letting your body get into the groove can really help.
Another thing you can do at home is experiment with different positions for vaginal intercourse, especially ones that allow you to be the person that controls movement. There are some great ideas (and illustrations!) on The American Cancer Society’s website.
Sexual aids can also help. Using pillows or specialized cushions for positioning can change the angle and improve comfort. Ohnut is another inventive product that can reduce pelvic discomfort with vaginal intercourse by allowing women and their partners to use stretchy, cushy rings to buffer against deep penetration.
Additionally, if vaginal intercourse hurts, think outside the box! There are lots of fun and sexy things to do that don’t involve penetration. Check out some ideas from the experts at A Woman’s Touch.
Try over-the-counter (OTC) vaginal moisturizers and personal lubricants.
Non-prescription topical options are first-line treatment for survivors experiencing sexual discomfort due to vulvovaginal atrophic changes and dryness (Carter et al., 2018; NCCN, 2021). These include regular maintenance with vaginal moisturizers, and the use of personal lubricants with sexual activity.
To learn more, check out the article on the Vulvovaginal Blues (authored by yours truly) that appeared in an earlier issue of Elephants and Tea.
Consider pharmacologic interventions.
Prescription options for treating sexual pain related to vulvovaginal atrophic symptoms are available, including topical estrogens, topical androgens (DHEA or prasterone), topical anesthetics (lidocaine), and oral medications (ospemifene) (Carter et al., 2018; NCCN, 2021). Some of these treatments do not have a lot of data regarding their safety and effectiveness in cancer survivors and AYA populations, however. If OTC options haven’t worked for your symptoms, have a discussion with your provider about what might be appropriate for you.
Pelvic floor physical therapy.
I swear to you that your friendly local pelvic floor physical therapist just might become your new best friend! In my opinion, these professionals are the most underrated of the essential members on any cancer survivor’s sexual healthcare team.
Generally speaking, physical therapists (PTs) specialize in helping people restore and maintain movement and physical function after illness and injury. Pelvic floor physical therapy is (you guessed it) a specialty area that focuses on rehabilitating pelvic floor function. These PTs work with both men and women to address problems like pelvic pain, sexual dysfunction, and bowel and bladder incontinence.
Pelvic floor physical therapists can assess sexual and pelvic pain and utilize a variety of therapeutic techniques to improve symptoms. These can include strengthening exercises, muscle relaxation techniques, manual tissue manipulation and massage, as well as mind/body and breathing techniques, biofeedback, and vaginal dilator therapy.
Vaginal Dilator Therapy (VDT).
VDT is both a preventive technique and a treatment option for different causes of sexual pain. After pelvic radiation, VDT can help prevent the formation of adhesions, when the mucosal tissues on either side of the vaginal walls become stuck together. DVT can also help prevent vaginal stenosis (that narrowing, shortening, and loss of elastic stretchiness), which can develop after radiation, surgery, or with hormone changes. VDT is also used to assist women in learning how to control and relax the muscles around their vaginal entrance, promoting more comfortable intercourse.
The purpose of VDT is to regularly separate the walls of the vagina, and to stretch the vaginal tissue and the pelvic floor muscles. A VDT session consists of inserting a cylindrical plastic or rubber tube (they come in multiple, graduated sizes and sometimes even fun colors) into the vaginal canal and leaving it in place for a specified amount of time (usually a matter of minutes). Someone on your healthcare team (your doctor, nurse, or pelvic floor PT) should provide education and a demonstration of the technique, along with specific instructions to follow regarding the duration and frequency of the therapy. Usually, after these initial instructions, women can complete these exercises at home. To be effective, VDT should typically be done at least 3-4 times a week.
Vaginal dilators are considered medical devices and can be purchased online, and your insurance may cover the cost. Ask your healthcare team for recommendations. For more details on how to use a vaginal dilator, check out Memorial Sloan Kettering Cancer Center’s website.
Bottom Line
Sexual pain after cancer is a common experience, but it shouldn’t be something you feel like you have to suffer through! There are a lot of options for managing and improving these symptoms. Ask your provider for help in determining what may be causing them, so that you can find a way to change that pain back into pleasure again.
Check out these resources!
References and Bibliography:
American Cancer Society. (2021). Managing female sexual problems related to cancer. https://www.cancer.org/treatment/treatments-and-side-effects/physical-side-effects/fertility-and-sexual-side-effects/sexuality-for-women-with-cancer/problems.html
Bachmann, G., & Santen, R. J. (2021, May 25). Genitourinary syndrome of menopause (vulvovaginal atrophy): Treatment. UpToDate. https://www.uptodate.com/contents/genitourinary-syndrome-of-menopause-vulvovaginal-atrophy-treatment
Bober, S. L., & Krapf, J. (2021, June 18). Overview of sexual dysfunction in female cancer survivors. UpToDate. https://www.uptodate.com/contents/overview-of-sexual-dysfunction-in-female-cancer-survivors
Carter, J., Lacchetti, C., Andersen, B. L., Barton, D. L., Bolte, S., Damast, S., Diefenbach, M. A., DuHamel, K., Florendo, J., Ganz, P. A., Goldfarb, S., Hallmeyer, S., Kushner, D. M., & Rowland, J. H. (2018). Interventions to address sexual problems in people with cancer: American society of clinical oncology clinical practice guideline adaptation of cancer care Ontario guideline. Journal of Clinical Oncology, 36(5), 492–511. https://doi.org/10.1200/JCO.2017.75.8995
National Comprehensive Cancer Network. (2021). NCCN clinical practice guidelines in oncology: Survivorship [Version 1.2021]. https://www.nccn.org/professionals/physician_gls/pdf/survivorship.pdf
Shifren, J. L. (2020, July 16). Overview of sexual dysfunction in women: Management. UpToDate. https://www.uptodate.com/contents/overview-of-sexual-dysfunction-in-women-management
Vaginismus. (n.d.). What causes vaginismus? Retrieved on July 20, 2021, from https://www.vaginismus.com/causes-of-vaginismus
Wincze, J. P., & Weisberg, R. B. (2015). Sexual dysfunction: A guide for assessment and treatment (3rd ed.). The Guilford Press.



Join the Conversation!
Leave a comment below. Remember to keep it positive!